|
|
||
|
|
Recently,
in our little group, a good deal of discussion has taken place with regard
to the relationship of Bartters Syndrome to Gitelmans Syndrome.
Gitelmans has been called a division or variation of Bartters and Bartters
has been described similarly in its relationship to Gitelmans.
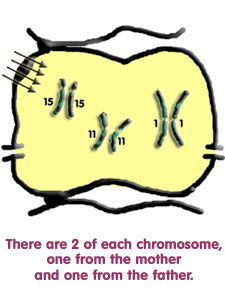
They are genetically quite different but unfortunately have one thing
in common and that is the loss of salt NaCl. This
loss, of course, leads to other electrolyte losses. The chromosomes involved
are shown below.
(But please note: they are not really lying loose in the cells, but are inside the nuclei!) |
|
|
|
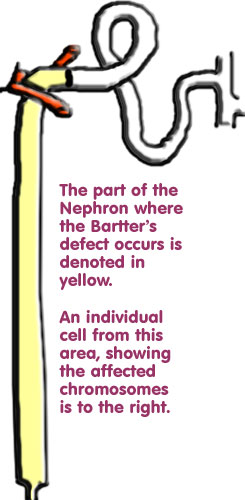
Bartters may result from a defect in one of several chromosomes. Look back to page 4 and note that this syndrome commonly is caused by the malfunction of either the transporter or the channel that recycles potassium or the chloride channel. Each of these is programmed by a different gene on a different chromosome. For the animated drawing, go to page 6 to view normal functioning. |
 |
|
The gene for the transporter is on chromosome 15, for the potassium channel on chromosome 11 and for the chloride channel on chromosome 1. (There is another gene on chromosome 1 where a rare defect causes Bartter's syndrome accompanied by congenital deafness.) If even one of these defects is present the whole transporting system breaks down and Bartters syndrome results. |
||
|
|
||
|
|
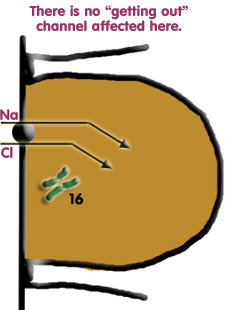
Gitelmans is due to a defect on chromosome 16. This affects the transporter that takes sodium and chloride into cells in the distal tubule. A source of confusion lies in the fact that it has been stated that there are many different types of Gitelmans. In general, what is meant is that many different mistakes or variations occur in the DNA that leads to the formation of the transporter. The end result is the same, a defective transporter. Similarly, mistakes may occur in any of the Bartters chromosomes. |
 |
|
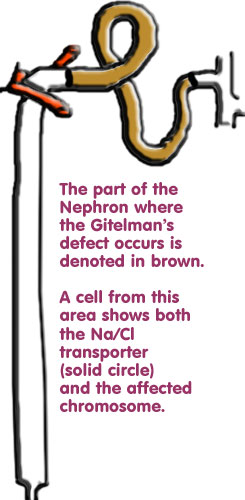
Using these drawings to illustrate Gitelmans we note the defect to occur distally. But it is important to note that the defect described in Bartter's does not occur in Gitelmans. The transporter and channels affected by Bartters are present and working in Gitelmans but you might say that they dont have much salt to work on!!! Even so prostaglandins do not always rise because other factors induce renin increase. |
||
| |
Note that in Bartters the tubular defect found in Gitelmans also does not occur. Still, the amount of salt pouring down from above is far too much for the distal system to handle. Similarly, in Gitelmans the defect found in Bartters does not occur. Although a good deal is known about how salt is treated normally in the body, especially by the renin-angiotensin-aldosterone system (RAAS), no good explanation exists as to why magnesium is often lost when different defects occur. The RAAS is concerned with things like sodium, potassium and chloride, all of which have the valency of 1. Where this system crosses paths with calcium and magnesium both of which have a valency of 2 is not understood although some theories have been put forward. |