![]()
![]()
|
|
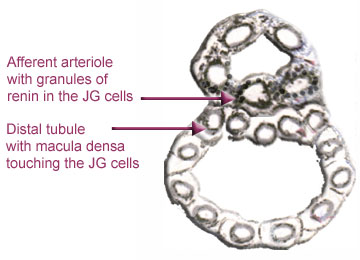
The last diagram shows how sodium, potassium and chloride are normally transferred through the cells of the thick ascending limb and back into the blood. In Bartters because the normal transfer is not going on, this abnormal load of electrolytes enters the distal tubule and the collecting ducts. Even though the distal tubule itself is short it contains several types of cells and soon we discover the dire consequences of this overwhelming load. We have entered a jungle and there be dragons ahead.
|
Distally the tubules are submerged by this surfeit of ions. A large part of the sodium, potassium and chloride is lost to the body and the loss of potassium is made worse by the exchange of sodium for the bodys precious potassium under the influence of aldosterone. Other changes occur as well but these will be discussed later. (Were chicken.) |
|
|
|
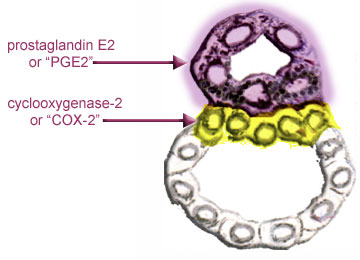
If we colour COX-2 yellow and PGE2 mauve the diagram above may be represented as below:
Now you can see how Celebrex and similar anti-inflammatory drugs work. COX-2 is inhibited and so is the PGE2. PGE2 cannot start the process of renin formation which leads to the production of aldosterone and many of the symptoms of Bartters syndrome vanish. Sometimes these comparatively new drugs have side effects and in addition most or all patients must take a potassium supplement and often magnesium as well. If you are wondering what happens when there is high salt at the macula densa, these cells become ATP/adenosine producing cells. More about how the renin-angiotensin-system works next week. |
[Previous
Page] [ 1 ] [ 2
] [ 3 ] [ 4 ]
[ 5 ] [ 6 ] [ 7
] [
8 ] [ 9 ] [ 10
] [ 11 ] [ 12
] [ 13 ] [Next
Page]
[
Lyn's Dedication Page ]