![]()
![]()
|
|
If you look back at the pictures of the nephron, you will note that the descending and ascending limbs of the loop of Henle run side by side. Note that the proximal tubule gives rise to the descending limb and the thick ascending limb becomes continuous with the distal tubule.
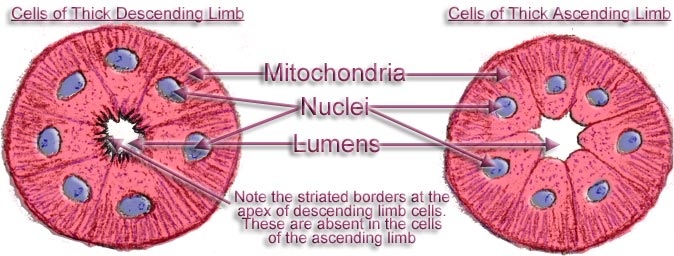
Here are diagrams of the cell types of the thick descending and thick ascending limbs of the loop as seen by light microscopy.
|
|
|
|
The striated borders at the apex of the cells of the descending loop give the cells a greater area for the reabsorption of filtrate, while the striations at the base are formed by mitochondria vital for the energy production of the cell. In all, these descending loop cells tend to act like the cells of the proximal convoluted tubule. HOWEVER, ITS A MUCH DIFFERENT STORY WHEN IT COMES TO THE CELLS OF THE THICK ASCENDING LIMB. These cells look like the cells of the distal tubule but how different they are! For it is in defects in these cells that all the causes of Bartter's Syndrome lie. No one could have found these by looking down a microscope and only by the wonders of modern biochemistry and genetics were they discovered. Consider the unbroken circle of cells lining the thick ascending loop of Henle. Then think of the whole of the ascending limb lined with these cells. Now look at the single cell in which the transporter and the channels are indicated. (This diagram is intended to illustrate only occurrences in Bartters syndrome and all other cell activities are omitted.) |
What we have called the hand of Donald Duck is called scientifically the NKCC2, the Bumetanide-sensitive Na-K-2Cl cotransporter (BSC). A defect here causes Bartters syndrome Type I.
The “Rob Peter to pay Paul” channel is called the ROMK channel and also the “Inwardly rectifying potassium channel.” A defect here causes Bartter’s syndrome Type II.
The Getting Out channels that take chloride out of the cell into the interstitial tissue are called the ClC-Kb and the ClC-Ka channels. Defects here causes Bartters syndrome Type III. ClC-Kb is the more active channel. A more complicated defect involving both channels can cause Bartter's syndrome Type IV.
Type IV Bartter's is caused by a defect in a substance called Barttin which is associated with both the ClC-K channels. Patients with this defect are deaf.
X marks the spot of the Calcium sensing receptor (CaSR), where a defect causes Bartter's syndrome Type V.
Unfortunately, not all scientific organizations use the same lettering – but just think of Donald Duck and his friends and you’ll be safe.
AND SO a defect in any one of these five movers of ions, as they are more scientifically called, causes Bartter’s syndrome. The amount of sodium, potassium and chloride that is unable to be reabsorbed is so large that it runs into the distal tubule and collecting ducts with disastrous results because these tubules just cannot cope with it.
This will be discussed next week.
I know that you are asking “Why is magnesium lost?” That’s the $64 question. Normally biochemical reactions and electrical potential differences carry magnesium between the cells and through to the blood. But when these reactions do not occur, why do many Bartter’s patients have no problem with magnesium at all?
[Previous
Page] [ 1 ] [ 2
] [ 3 ] [ 4 ]
[ 5 ] [ 6 ]
[ 7 ] [ 8 ] [
9 ] [ 10 ] [ 11
] [ 12 ] [ 13
] [Next
Page]
[
Lyn's Dedication Page ]