|
|
|
|
Because a great many of the symptoms and signs of both Bartters and Gitelmans syndromes are due to the overproduction of renin in the juxtaglomerular cells (JG cells) a more in depth study of the renin-angiotensin-aldosterone system must be made. Before going on with this it was decided to root out the old slides and pictures in the cellar and have a holiday looking at juxtaglomerular cells. It is doubtful if similar slides are made today because when these were made over forty years ago Bartters syndrome had just been discovered and the discovery of Gitelmans syndrome was in the future. There was consequently no treatment for Bartters syndrome beyond replacing potassium and the use of spironolactone. It proved to be no holiday and the slides were full of dust and heaven knows what.
This recent diagram is included for orientation:
| While we admit this picture is not artistic, it shows the relationship between the macula densa and the JG cells. (See previous page) See also the diagram on page 3. The JG cells contain more granules than are usually found inside a normal kidney. | 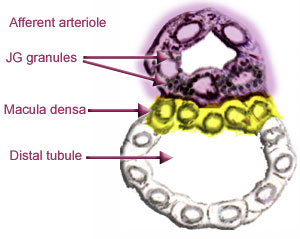 |
|
|
||
|
|
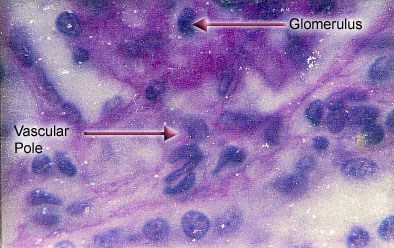
Slide 1
Here is the vascular pole of a normal glomerulus in an eleven month old child. Note the absence of juxtaglomerular granules. There is no evidence of hypertrophy.
|
|
|
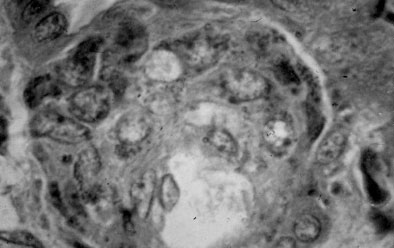
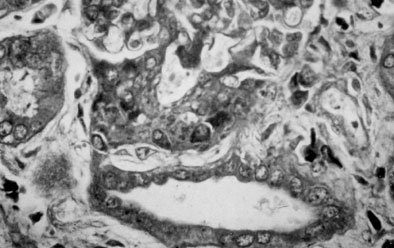
Slide 2 Here is an enormous field of granulated JG cells in the wall of an afferent arteriole in a child with Bartters syndrome. (The year was about 1963.) This child was one year of age and was resistant to treatment with potassium supplements and spironolactone. We did not know until it was too late that the child was losing large amounts of magnesium. |
 |
| Our department was in regular contact with Dr. Bartter who was unable to help us as apparently none of his patients required extra magnesium. In 1962 when Dr. Bartter wrote his paper, very little thought was given to routine magnesium testing. Besides this almost no nonsteroidal antiinflammatory drugs existed and nobody had used them in Bartters syndrome. |
 |
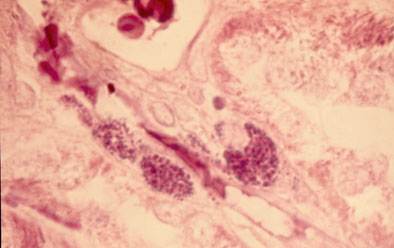
Slide 3
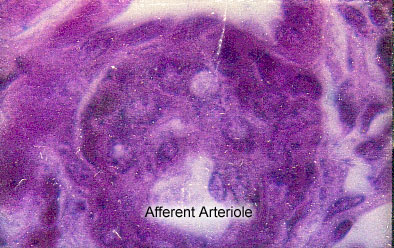
Another section from the same patient. The glomerulus is above, JG-cells in the centre and macula densa and distal tubule below. Between the JG-cells and macula densa are large vacuoles. |
|
|
Slide
4
This is a colour transparency of Slide 2 (that survived). It shows JG granules stained by the Bowie method. |
 |
 |
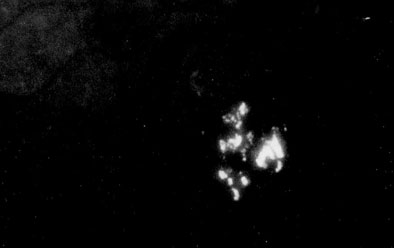
Slide 5
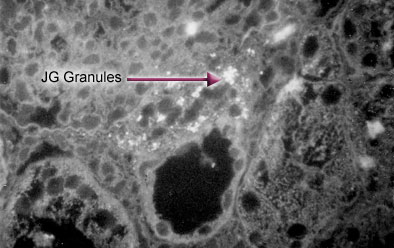
Renin stored in granular form is inactive, yet it is possible to make an antibody to it (truthfully more by good luck than by good design.) If the antibody is combined with a fluorescent dye and the tissue is examined by ultraviolet light the JG granules will shine out of the darkness. Here is a section of the kidney in the above case stained with such an antibody. |
|
|
|
Slide
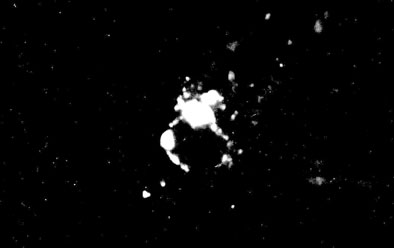
6
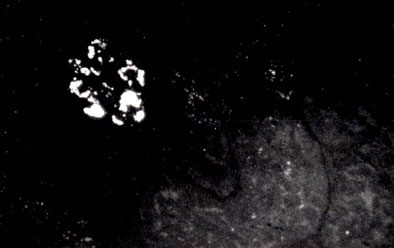
Here is a similar section from a rabbit. The faint outline of the glomerulus has long since faded but the JG granules still shine. Their crescent outline shows them to be crowded around the nuclei of the JG cells. |
 |
 |
Slide 7
A slide
similar to slide 6 but this rabbit was salt deficient. Note the
increased granulation of the JG cells. |
|
|
Slide
8
JG granules in adult pig. |
 |
|
|
Slide
9
JG granules in a salt deficient dog. |
|
|
Slide
10
Note the heavy granulation of the JG cells in a dog suffering from high output heart failure due to an arteriovenous fistula. The normal dog kidney was not found to have many prominent JG cells. |
 |
By this technique, we were able to stain JG granules in human, rabbit, pig and dog kidneys but were unable to stain JG granules in the rat.
Next
week we will look at the normal renin-angiotensin-aldosterone system and note
how it malfunctions in Bartter's and Gitelman's syndromes. It was soon
noted (by Bartter) that despite the large amounts of renin produced, particularly
in Bartter's syndrome it was not accompanied by a rise in blood pressure.
Rather the blood pressure was normal or low. In an animal that is salt
deficient, large amounts of renin also accumulate and yet the blood pressure
does not rise. Many people with hypertension improve with a lower salt
intake.
In an animal with large kidneys, even the size of a rabbit's, you can look at
fields of well granulated JG cells under the microscope but will be unable to
tell how much renin there is in the entire kidney. In the rat, however,
the kidneys are small and you can make cuts through an entire kidney and mount
the tissues on microscope slides. If you stain the granules you will be
able to make an estimate of the amount of renin present or at least be able
to compare one kidney with another.
A good many years ago, Dr. Lewis K. Dahl of Brookhaven developed two strains
of rat, one resistant to salt induced hypertension and one sensitive.
We were lucky enough to study the two strains of rat and found that rats with
a lot of JG granules had much lower blood pressures and healthier arteries than
those with fewer JG granules.
Three of us presented these findings at the "Spring Meetings" of the
Biologists in Atlantic City in 1969. At that time, these findings were controversial
and were greeted with some scepticism because many people associated elevated
renin with hypertension.
After going through the debris in the cellar we were only able to find two transparencies.
One showed the normal glomerulus of a rat of a resistant strain eating a high
salt diet. The other shows the greatly increased numbers of granulated
JG cells when a similar rat was fed a salt deficient diet.
|
|
Slide
11
Here is the glomerulus of a rat, resistant to salt induced hypertension and eating a high salt diet. It is stained a bit differently from its companion, but believe me: It is normal and had small normal JG cells. |
 |
|
|
Slide
12
This glomerulus is from a healthy rat of the resistant strain eating a diet deficient in salt. Note the enlarged and heavily granulated JG cells in the afferent arteriole. |
The story above was a happy story but now I will tell you a rather sad one.
This will help to explain why renin got its bad reputation because in some diseases
and surgical conditions it can cause lethal hypertension. Dr. Goldblatt,
who was a nephrologist at the Cleveland Clinic showed that if one renal artery
was constricted (whether by disease or by experimental means) large amounts
of renin would accumulate in its JG cells. The blood flow to the "Goldblatt"
kidney was therefore low and the pressure on the arteries in the kidney was
also low. Although people did not realize this at first, this was a "protected"
kidney. On the other hand, the opposite kidney, subjected to high blood
pressure because of the large amounts of renin pouring into the circulation
would eventually be destroyed.
Unfortunately, a small child with a congenital constriction of one renal artery
came to surgery. I don't know the entire history but one of the doctors
gave me a piece of the kidney that they removed. Wouldn't you know?
They had removed the Goldblatt kidney. Maybe they couldn't repair the
artery. Who knows?
|
|
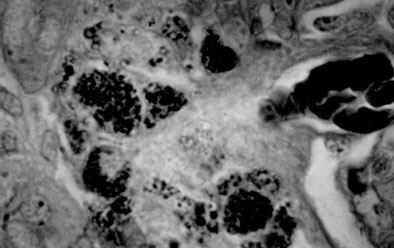
Slide
13
Here is a section of the kidney stained to show the JG cells and granules. I wonder if the child eventually had to have a transplant? |
 |
On
a lighter vein we found JG cells in the Director's pet budgie, his pet guppy,
in the primitive kidney of pig embryos and in both fresh and salt water fish.
Why would a salt water fish need JG cells to retain salt? I wonder if
the fish was losing salt via its gills. (P.S. The Director kept the cat
away from us.)
Next week we will have to get down to business.
|
[Previous
Page] [ 1 ] [
2 ] [ 3 ] [
4 ] [ 5 ] [
6 ] [ 7 ] [ 8 ]
[ 9 ] [ 10 ]
[ 11 ] [ 12 ]
[ 13 ] [Next
Page] |